One of the greatest personal “take homes” from #ECC2015 was a far better understanding of the latest round of Melanoma drugs.
One of the greatest personal “take homes” from #ECC2015 was a far better understanding of the latest round of Melanoma drugs.
You need to know that I didn’t go to ECCO thinking I would be given a fix….I didn’t expect to be told of a magic cure. I kept hearing about all of these amazing discoveries & advancements but I couldn’t really comprehend what they mean for me because as yet (find a piece of wood) I have no need for drugs.
To understand the latest treatment options you need to go backwards slightly.
Melanoma isn’t new, there are references to and examples of it for hundreds of years, however it wasn’t until 1968 that there was any start to actually look at and address Melanoma as being different to other cancers. But even then it was so rare and the understanding of it was so limited that very little progress was made. They would treat melanoma as they did with do many other Cancers – Chemotherapy – and it wasn’t working.
Once “we” eventually started treating Melanoma as a Cancer in its own right, it became clear that this unique Cancer was going to prove tricky. Drugs would work on some patients not others, patients would seem to respond but then randomly the drug would stop working & in some cases the disease would almost seem to have been sped up – moved up a gear or two dozen in aggression.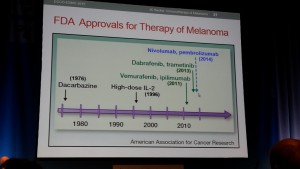
This timeline of available drugs shows that in recent years there are quite a few new drugs entering the scene. The media have reported this too…..”apparently these new drugs are the cure”…but really they are just the first step forward & in the right direction, in a very long journey.
Prior to 2010 options were limited & the side effects were significant. As these new drugs come along each brings a potential ….we will live longer…we hope. Wonder drugs sometimes come with a sting in the tail in the form of side effects….but we are used to that. Patients weigh off risk of not having a drug at all with risk of how great the side effect is….and who decides… it isn’t the patient.
These drugs need to be tested. Let’s take niavity out of the frame immediately by accepting that the testing of these drugs start in Clinical settings & in mice. Once they are deemed to show the indicated response they get licenced for Human use. Then the testing of these drugs falls to trials. These clinical trials are divided up into Phases and they must get passed each phase before they eventually get approved as a treatment.
Phase 1 trials are the first point at which a trial is given to a patient. Most Phase 1 trials are with Stage 4 patients…for whom these drugs are the “last hope”. The Phase 1 trials are to test if the drug is actually safe on humans & what the side effects are…. It’s a voyage of discovery…the human guinea pigs that gamble with adverse effects in the hope that a drug might give them time.
The number of patients on a Phase 1 trial is limited, and because of how advanced their disease already is they often don’t make it through the clinical trial – not because of the drug itself not being any good…but because it took too long or their immune system couldn’t cope.
Please remember – we are still talking about Melanoma here & at this moment in time once you get to a certain stage without the blessing of a positive response to a drug, death is inevitable.
The later stage Phase 2 or 3 trials look at the in depth comparisons between existing drugs, combinations of drugs & the change this has on side effects. A drug can get through to Phase 3 and then not get approval – generally by this point for financial reasons – but that is another blog post.
There are a few drug options out there now. Some are better than others…most patients find that the only way to get treatment for Melanoma is on a trial..so for us, even more than the side effects we are interested in 3 particular things; Response rate, progression free survival (the time you get on a drug before resistance) and overall survival.
Response rate means the number of patients given a drug that it actually seems to work for – Chemo had a response rate of 4%…Vemurafenib had a response rate of 54%..Ipi’s response rate is a lowly 11%….Pembro’s response rate is around 38-40% – I say around because with this one it depends where your disease has progressed…16% for liver metastasis but amazing 64% for lung mets.
Confused yet? It’s very complicated…I needed help from my friends Gilliosa & Violetta to clarify stats I didn’t understand (xxx).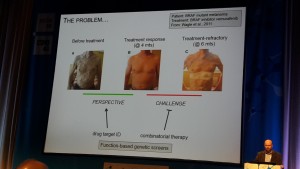
Vemurafenib looks on paper to be a great drug…for a while it can have great results…but then enter PFS (progression Free Survival)…and sadly Vem (also known as Zelboraf) generally stops working between 6-9 months.
Ipiluminab has a poor RR…and worse still it has some pretty horrid side effects….but the overall survival is at about 47% for 1 year and 25% for 2 years.…that would be 25% of the patients given Ipi are still alive 2 years later…which from a treating melanoma perspective is great news.
The latest drugs are known as Immunotherapy drugs…and Ipi is one of these…it’s arrival in 2011 has changed the history of Melanoma.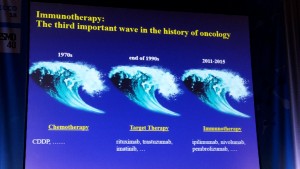
The simple fact of the matter is that an Immunotherapy drug alone will never kill or cure a cancer completely. Cancer tumours use the body’s immune system to protect themselves and these new drugs are engineered to confuse the immune system. Combining radiotherapy with immunotherapy helps the drug to work more effectively, but one oncologist at ECCO suggested taking this thought one step further and introducing Virotherapy to then take the drug & it’s positive impact on the tumour & spread it around.
There are new trials ongoing…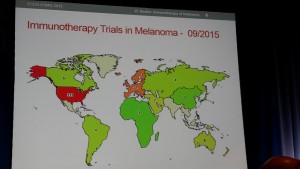 (37 immunotherapy trials currently running across Europe)…targeted therapy…and combining targetted therapy drugs…and into Biomarkers which are tools which help to pinpoint who will respond to the Immunotherapy drugs or not & why. Every single patients Melanoma experience is different.
(37 immunotherapy trials currently running across Europe)…targeted therapy…and combining targetted therapy drugs…and into Biomarkers which are tools which help to pinpoint who will respond to the Immunotherapy drugs or not & why. Every single patients Melanoma experience is different.
Research, research & more research…its ongoing & its vital.
We think these wonder drugs are the light in the tunnel because some of them don’t have hideous side effects and others seem to hold off any progression for several years…but we just don’t know everything yet.
We don’t know what happens if & when those drugs stop working – Melanoma is instinctively adaptive & it will find a way to fight…to resurface in a new hybrid version of its former self…seemingly impenetrable.
In the meantime we face barriers of money…a drug might get licensed for use…but it isn’t accessible….which seems very wrong...